
Discover how process automation in healthcare can streamline tasks, reduce errors, and improve patient care. Transform your facility today!
TL;DR:
- Process automation in healthcare reduces manual workload by streamlining repetitive tasks through reliable digital workflows. Successful implementation requires organization-wide readiness, clear process mapping, and system-level integration for scalability and sustainability. Embedding automation into enterprise infrastructure prevents failures caused by isolated task automation or system updates.
Administrative overload is real. Staff are buried in paperwork, prior authorizations pile up, and patients wait longer than anyone wants. Growth-stage hospitals and clinics feel this pain sharply. Every manual handoff is a chance for error, delay, or burnout. Process automation changes that equation. It shifts repetitive, rules-based tasks off your team’s plate and into reliable digital workflows. This guide walks you through exactly how to build that shift, step by step, without the guesswork or expensive missteps.
Key Takeaways
| Point | Details |
|---|---|
| Automate rules-based steps first | Start with intake, eligibility, and authorization tasks before scaling to end-to-end orchestration. |
| Establish process readiness | Assess your EHR system, stakeholder buy-in, and workflow documentation before launching automation. |
| Prioritize system-level orchestration | Embed automation within enterprise infrastructure to avoid workflow breaks and maximize ROI. |
| Measure and iterate continuously | Track outcomes like error rates and turnaround times, using results to refine and expand automation. |
Understanding process automation in healthcare
Process automation in healthcare means using software to handle repeatable administrative and clinical tasks automatically, based on predefined rules, without needing a person to trigger each step. Think eligibility checks that run on their own, appointment reminders that fire at the right time, or discharge summaries that route to the right team instantly.
The goal is straightforward. Reduce manual workload. Cut turnaround times. Increase accuracy. That’s the core of what automation benefits in healthcare actually delivers.
A few key terms are worth knowing before moving further:
- EHR (Electronic Health Record): Your digital patient data system. It’s the backbone of most automation workflows.
- Rules-based workflow: A process that follows fixed logic. “If patient X meets criteria Y, trigger action Z.” No judgment calls needed.
- Orchestration: Coordinating multiple automated steps so they work together as a single end-to-end process, not isolated tasks.
- Prior authorization: The insurance approval step before a treatment or medication is dispensed. A notorious time sink. A prime automation target.
Right now, the most active automation focus areas in healthcare operations include patient admissions, bed and capacity management, discharge coordination, insurance eligibility, and follow-up scheduling. End-to-end patient flow automation is increasingly implemented as an integrated operating model that aligns admission planning, capacity management, staffing, discharge coordination, and care progression all in one connected system.
Here’s a quick look at where automation typically delivers the most impact:
| Focus area | Typical manual pain point | Automation impact |
|---|---|---|
| Admissions planning | Manual bed checks and calls | Faster placement, fewer delays |
| Insurance eligibility | Manual portal logins per patient | Real-time checks, fewer denials |
| Prior authorization | Fax-based approvals | Faster approvals, lower abandonment |
| Discharge coordination | Fragmented team communication | Standardized handoffs, shorter stays |
| Follow-up scheduling | Phone tag with patients | Automated reminders, higher show rates |
Pro Tip: Before picking a tool, map your current workflow on paper or a whiteboard. You’ll almost always find the biggest bottleneck isn’t where you assumed it was.
Preparing your organization: prerequisites and readiness
Clear understanding of what automation can do is just the start. The harder question is whether your organization is ready to actually implement it.
Readiness has two sides: technical and organizational. A clear-eyed assessment of both will save you months of frustration later.

On the technical side, ask these questions. Is your EHR mature and well-configured? Are your current processes documented anywhere, or do they mostly live in people’s heads? Does your IT team have bandwidth to support integrations?
On the organizational side, governance matters enormously. Who owns each process? Who approves changes to workflow rules? Without clear answers, automation projects stall in committee or get quietly abandoned after the pilot.
The methodology that actually works for growth-stage hospitals and clinics is consistent: start with workflow mapping and value-stream thinking, automate the most stable and rules-based steps first, like intake, eligibility, status checks, and prior authorization, and only then scale to broader end-to-end orchestration. This approach, supported by process improvement strategies from operations research, keeps early wins achievable.
Here’s a quick comparison of what’s required at different levels of automation:
| Requirement | Task-level automation | System-level automation |
|---|---|---|
| EHR integration | Basic API access | Deep, bidirectional data sync |
| Process documentation | Single workflow documented | All connected workflows mapped |
| IT support | Part-time support adequate | Dedicated integration resources |
| Governance | Team lead ownership | Cross-functional steering committee |
| Change management | Team training | Organization-wide adoption plan |
Common readiness gaps include:
- Undocumented workflows: Automation can’t run on “how we’ve always done it.” Processes need to be written down first.
- Siloed IT and operations: When IT and clinical ops don’t communicate, integration projects drag.
- No success metrics defined: If you don’t know what “better” looks like before you start, you won’t know if the automation actually worked.
- Exception-heavy processes: Workflows full of special cases are hard to automate reliably. Start with the clean, predictable ones.
Pro Tip: The best first automation target has three qualities. It’s high volume, it follows clear rules every time, and it has a measurable outcome you can track before and after.
Step-by-step: Building a process automation project
With organizational readiness established, you’re ready to move through the actual steps that bring your automation plan to life. This isn’t theory. This is the sequence that actually gets results.
Phase 1: Map the process Document the target workflow from start to finish. Every step, every handoff, every system involved. Include what happens when something goes wrong. Don’t skip the exceptions just because they’re messy.
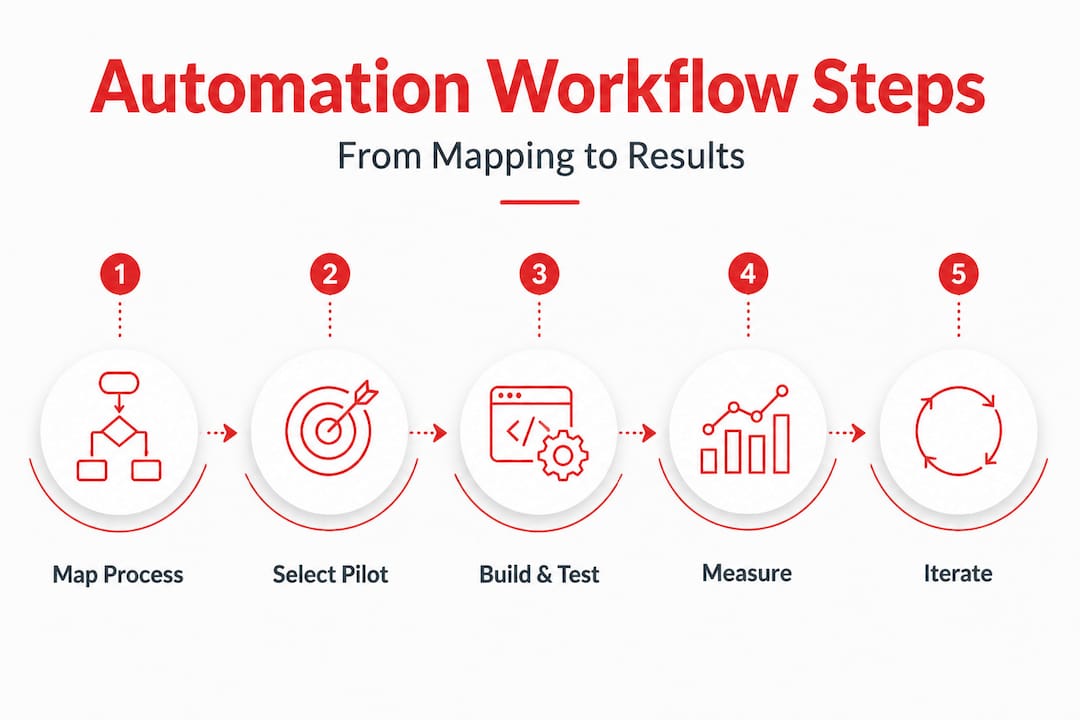
Phase 2: Select the pilot step Pick one discrete, rules-based step within the mapped process. A single decision point, not a whole workflow. Eligibility checks are a great first pilot. So is a simple appointment reminder sequence.
Phase 3: Build and test Build the automation with your EHR or workflow tool. Test it with real scenarios, including edge cases. Get feedback from the staff who actually use the process. Adjust before you go live.
Phase 4: Measure and iterate Track your baseline metrics against post-automation results. Look at time saved, error rates, and staff feedback. Make adjustments based on data, not opinions.
Phase 5: Scale up Once the pilot step is stable, expand to adjacent steps in the same workflow. Then move to the next workflow. This is how you build toward full orchestration without blowing up your operations.
A practical checklist for what to automate first:
- Insurance eligibility verification
- Prior authorization submission and status checks
- Follow-up appointment scheduling
- Patient intake forms and data capture
- Lab result routing and notification
- Discharge checklist completion tracking
The data on prior authorization is striking. Prior authorization automation can measurably improve denials and appeals rates and reduce prescriber abandonment when payer-criteria checks are automated using EHR-derived data. In real implementations, prescriber abandonment drops from 22% to as low as 4%. Denial rates fall by around 11%.
| Metric | Before automation | After automation |
|---|---|---|
| Prior auth denial rate | ~18% | ~7% |
| Prescriber abandonment rate | 22% | 4% |
| Average authorization time | 3-5 days | Same day or next day |
| Staff hours per auth | 45 min | Under 10 min |
For more advanced use cases, integrating predictive AI in healthcare workflows opens up risk-based interventions. For example, EHR-integrated predictive AI can flag patients at high risk of readmission before discharge. Reducing readmissions through AI relies on EHR-integrated predictive AI and automated point-of-care decision support to standardize care and enable proactive outpatient management. This keeps patients out of the ER and your staff focused on prevention, not reaction.
Good workflow visibility best practices matter throughout this phase. You need dashboards that show where tasks are in the pipeline, not just whether the automation is technically running.
Pro Tip: Don’t pilot with a process that has lots of exceptions. Save those for later. Your first automation win should be clean and fast, so your team sees the value before skepticism sets in.
Verification and scaling: Measuring results and avoiding pitfalls
Once automated steps are running, verifying outcomes and learning from initial challenges is key to sustained improvement. This phase is where most organizations either lock in their gains or slowly watch the automation drift into disuse.
Start with the right metrics. Not just technical uptime. You want to track:
- Quality: Error rates, rework frequency, data accuracy
- Time: Average task completion time, wait times, turnaround
- Satisfaction: Staff and patient feedback
- Financial: Cost per transaction, denial rates, revenue cycle timing
Streamlining healthcare workflows over time requires consistent measurement. If you’re not tracking it, you can’t improve it.
The bigger risk isn’t a single task failing. It’s a task stalling quietly and nobody noticing. This is where system-level orchestration pays off. As one framework puts it:
“Many AI systems lack system-level execution. This causes failures when steps or data are incomplete.”
Automation delivers results only when it’s orchestrated at the system level, embedded into enterprise infrastructure, rather than treated as isolated task automation that fails when a step stalls or data is incomplete.
Common pitfalls to actively avoid:
- Automating exceptions: If a process is full of special cases, it’s not ready for automation yet.
- Ignoring manual workarounds: If staff have built unofficial fixes around a broken process, automating the official process won’t help.
- No end-to-end ownership: Every automated workflow needs one person or team responsible for it. Shared ownership usually means nobody’s watching.
- Skipping change management: Staff who don’t understand why the process changed will route around it.
- Treating automation as a one-time project: Workflows evolve. Automation rules need regular review.
Your CRM workflows in healthcare follow the same pattern. When patient relationship data lives in a siloed tool that doesn’t connect to your automation layer, the whole system breaks down at hand-off points.
Pro Tip: Embed automation into your core enterprise infrastructure from the start. Bolt-on automations break when systems update. Native integrations hold.
Why most healthcare automation fails—and how to break the pattern
Here’s something most vendor pitches won’t tell you: the majority of healthcare automation pilots quietly fail or plateau. Not because the technology is bad. Because the approach is wrong.
Task automation solves a visible problem in the short term. You automate the prior auth step and save hours immediately. That’s real. But then someone changes an insurance payer’s criteria. Or a new exception type appears. Or the EHR updates and the data field moves. The isolated task automation breaks. And without system-level oversight, nobody catches it until the damage is done.
The contrast is stark. Some healthcare leaders argue, and the evidence backs them up, that the next step is system-level execution embedded into enterprise infrastructure so that workflows advance end to end even when a step stalls or data is incomplete. That’s a fundamentally different architecture than patching individual tasks.
What we’ve seen consistently is that the organizations scaling sustainably are the ones who treat automation as a workflow redesign project, not just a software install. Their hard-won lessons:
- Redesign the process before automating it. Automating a broken process makes it fail faster.
- Invest in flexible infrastructure. Rigid automations break with every system update. Flexible ones adapt.
- Make ownership cross-functional. Clinical ops, IT, and administration all need a seat at the table. Not just IT.
- Measure continuously, not just at launch. Automation needs ongoing monitoring to stay effective.
- Plan for scale from day one. The system-level automation for clinics that grows with you is worth far more than a cheap point solution you’ll replace in 18 months.
The organizations that break the failure pattern share one trait. They stop thinking about automation as a list of tasks to check off and start thinking about it as an operating model. That shift is what separates a successful pilot from a system that actually scales.
Next steps: Partnering for effective healthcare automation
Armed with both practical instruction and big-picture perspective, here’s how to move from knowledge to action.
Scaling process automation is much easier with the right partner and the right tools from the start. You don’t need to figure out every integration yourself.
Rule27 Design’s Innovation Lab for healthcare automation helps growth-stage clinics and hospitals turn operational intent into automated, efficient systems that actually hold up under real-world conditions. We build custom admin panels, workflow tools, and integration layers that match how your team actually works, not how a vendor assumes you work. Whether you’re running a first pilot on eligibility checks or ready to build fully orchestrated patient flow systems, we help you move faster and avoid the mistakes that derail most automation projects. Our clients typically see 40% gains in operational efficiency. Let’s get yours moving.
Frequently asked questions
What are common starting points for process automation in hospitals?
Admission planning, eligibility checks, and prior authorization are ideal first steps since they rely on clear rules and consistent data. Patient flow automation increasingly covers all of these as part of a connected operating model.
How much can automation reduce administrative errors or delays?
Significant reductions are measurable quickly. Prior authorization automation alone can lower denial rates by 11% and cut prescriber abandonment from 22% to 4%.
How do you avoid automation failures in healthcare operations?
Embed automation into your enterprise systems rather than treating it as a standalone task. System-level execution ensures the workflow continues even if an individual automated step stalls or data is missing.
Is AI needed for initial healthcare automation projects?
No. Most early wins come from simple, rules-based workflows that don’t require AI at all. Predictive AI integration adds real value at later stages, particularly for readmission risk and proactive outpatient management.

About the Author
Josh AndersonCo-Founder & CEO at Rule27 Design
Operations leader and full-stack developer with 15 years of experience disrupting traditional business models. I don't just strategize, I build. From architecting operational transformations to coding the platforms that enable them, I deliver end-to-end solutions that drive real impact. My rare combination of technical expertise and strategic vision allows me to identify inefficiencies, design streamlined processes, and personally develop the technology that brings innovation to life.
View Profile

